


Revisiting the HIV theory of AIDS
Does HIV exist?

The discovery of ‘AIDS’ began in 19811 when a number of men in the U.S. were diagnosed with two relatively rare diseases, Kaposi’s sarcoma (KS), a type of cancer, and Pneumocystis carinii pneumonia (PCP), a fungal inflammation of the lungs. Although rare, KS and PCP were not new diseases, nor were either of them claimed to be caused by a virus; nevertheless, they became the first ‘AIDS-defining’ diseases. Subsequently, more diseases were added under the umbrella term AIDS.
The early research into these cases, which represented an abnormally high incidence of two otherwise rare diseases, indicated that they occurred almost exclusively within two ‘risk groups’, one of which comprised gay men with a very active sex-life. Their sexual activities were often accompanied by the use of ‘poppers’. Besides poppers, many other, likewise toxic, drugs were on the menu.
This highly toxic lifestyle was characterized by an extremely poor diet and a long-term intake of antibiotics.
‘Poppers’ are a type of drug that is inhaled; they are made from alkyl nitrites, which are carcinogenic.2 Kaposi’s sarcoma is a blood vessel tumor,3 and nitrite inhalants act on blood vessels.4

The majority of the early cases of KS were gay men who regularly inhaled ‘poppers’ and had done so for a significant period of time. The inhalation of toxic nitrites will cause damage to the respiratory system, including the lungs. The long-term toxic irritation of the lungs will produce a variety of symptoms that could also lead to a diagnosis of either pneumonia or PCP.
The other main ‘risk group’ comprised drug addicts, most of whom were intravenous drug users; the injection of toxic ‘illegal’ drugs will also produce serious adverse health effects.
It is clear that the first patients diagnosed with ‘AIDS’ were long-term consumers of a substantial quantity of toxic drugs, whether nitrites, antibiotics or ‘recreational’ drugs.
AIDS: What exactly is it?
The definition of AIDS (Acquired Immune Deficiency Syndrome) is anything but coherent. AIDS is not a specific disease at all, it is simply a collapse of the ‘immune system’ of a person said to be infected with HIV, characterized by a number of ‘opportunistic infections’.
HIV.gov5 states:

In contrast to other diseases, there is no universal definition of AIDS that could be used as a basis for sound statistics.
For developing nations, for instance, the World Health Organization introduced the “Bangui Definition”6 in 1986, with which many patients have been diagnosed with AIDS. According to this definition, anyone suffering from a few common and non-specific symptoms, like weight loss and diarrhea, is declared an AIDS patient (without blood tests, and thereby without HIV antibody tests).
In poor continents like Africa, where a third of the population is undernourished for decades, these symptoms are a well known mass phenomena.

Clearly, there is no specific illness that can be labeled ‘AIDS’; like so many other conditions, there are many causes and most of them are toxicological.
Virus causation
In 1983, Professor Luc Montagnier and his colleagues at the Pasteur Institute in Paris published a paper in Science, entitled Isolation of a T-Lymphotropic Retrovirus from a Patient at Risk for Acquired Immune Deficiency Syndrome (AIDS).7 This research led to Montagnier winning the Nobel prize for the discovery of HIV.
One year later, using similar methods, Robert Gallo and his colleagues repeated Montagnier’s experiments. Gallo is considered the co-discoverer of HIV, alongside Montagnier.
If there is an AIDS-causing retrovirus, the evidence in these 1983/84 publications should unambiguously confirm its existence.
Montagnier’s 1983 evidence:
Luc Montagnier took a sample from a sick patient said to have AIDS, and the sample was added to a cell culture. A number of chemicals were added including strong antibiotics and the highly oxidizing mitogen (a substance that increases cell division) PHA were added, and the culture was left on the bench for a few weeks.
The ‘discovery’ of HIV was then claimed to have been observed by:
Detection of a non-specific enzyme (reverse transcriptase activity, which is an enzyme to convert RNA to DNA).
A reaction between a few proteins.
An image of a few non-specific particles of unknown provenance, composition and biological function.
Luc Montagnier did not have proof that the enzyme activity and the reaction of a few proteins were due to a virus—because the enzyme and protein reaction is Montagnier’s proof of a virus (begging the question and affirming the consequent fallacy).
The enzyme activity8 and protein reaction9 are non-specific; meaning that they are not specific to any hypothetical ‘virus’. Thus making the explanation of a fictitious ‘virus’ as the culprit entirely unnecessary.
Some of the best known retrovirologists such Harold Varmus affirm that reverse transcription (the process created by reverse transcriptase) is non-specific:10

Montagnier did not have proof that the particles imaged in the electron microscope were viruses; the provenance, composition and biological function of the vesicles remained unknown. Research has shown that identical particles can be found in the majority of patients with enlarged lymph nodes not attributed to AIDS and at no risk for developing AIDS.11

He did not obtain the ‘virus’ in a pure and free state; separate from everything else. Without purification, one can not determine that the ‘virus’ exists at all, and the non-specific indirect laboratory results obtained from unpurified material are absolutely meaningless.
Gallo’s 1984 evidence:
In May 1984 Robert Gallo and his colleagues published four papers12 in Science with very few differences to Montaginer experiments. By December 1984, they also claimed to have characterized the HIV genome.13
His claims to have found the virus that was “the probable cause of AIDS” held no more validity than Montagnier’s, however, because he too failed to isolate and purify the alleged virus particles.
Gallo obtained non-specific genetic material from an unpurified mixture of fluid taken from a cell culture. This was then declared to be the HIV genome. However, there is no evidence that the genetic material was from a ‘virus’.
The Perth Group summarizes the genome experiments:14

If a scientist wishes to analyze the genetic material of an alleged ‘virus’, his first task is to obtain a mass of virus particles separate from everything else which also contains genetic material. That is, he has to isolate / purify the particles. However, this has never been done with ‘HIV’.
HIV testing
The most significant diagnostic tools for HIV/AIDS are:
1. Antibody tests
2. PCR
3. CD4 counts
These are what is known as surrogate markers. Surrogate means substitute – something that stands in place of something else, which means it has to be specific for that something else. These surrogate tests do not find a virus; rather, they find something else said to indicate the presence of a virus.
To validate a surrogate test, one must first do a careful study in which the surrogate is compared to the gold standard test. As an example, for a pregnancy test the gold standard would be the pregnancy itself. The only gold standard for HIV is HIV itself, that is, HIV isolation/purification.
However, as long as HIV has not been proven to exist, these tests cannot be calibrated for HIV – and they therefore not be used as tests for HIV. The specificity of these surrogate tests can be determined only by using HIV isolation as a gold standard. However, these surrogate tests have yet to be verified against the only suitable gold standard, viral isolation.
All tests for HIV are surrogate tests, which have never been compared to any gold standard; therefore, they are completely meaningless.
Antibody tests:
Since these so-called HIV antibody tests detect proteins and not the HIV directly, we have to assume that HIV must have been detected during the validation of the tests. Only then could one calibrate the antibody tests for this particular virus.
However, to date, nowhere in the AIDS scientific literature has there been any report whatsoever of the use of ’Human Immunodeficiency Virus’ itself as a gold standard for the verification of the sensitivity and specificity of the HIV antibody tests.
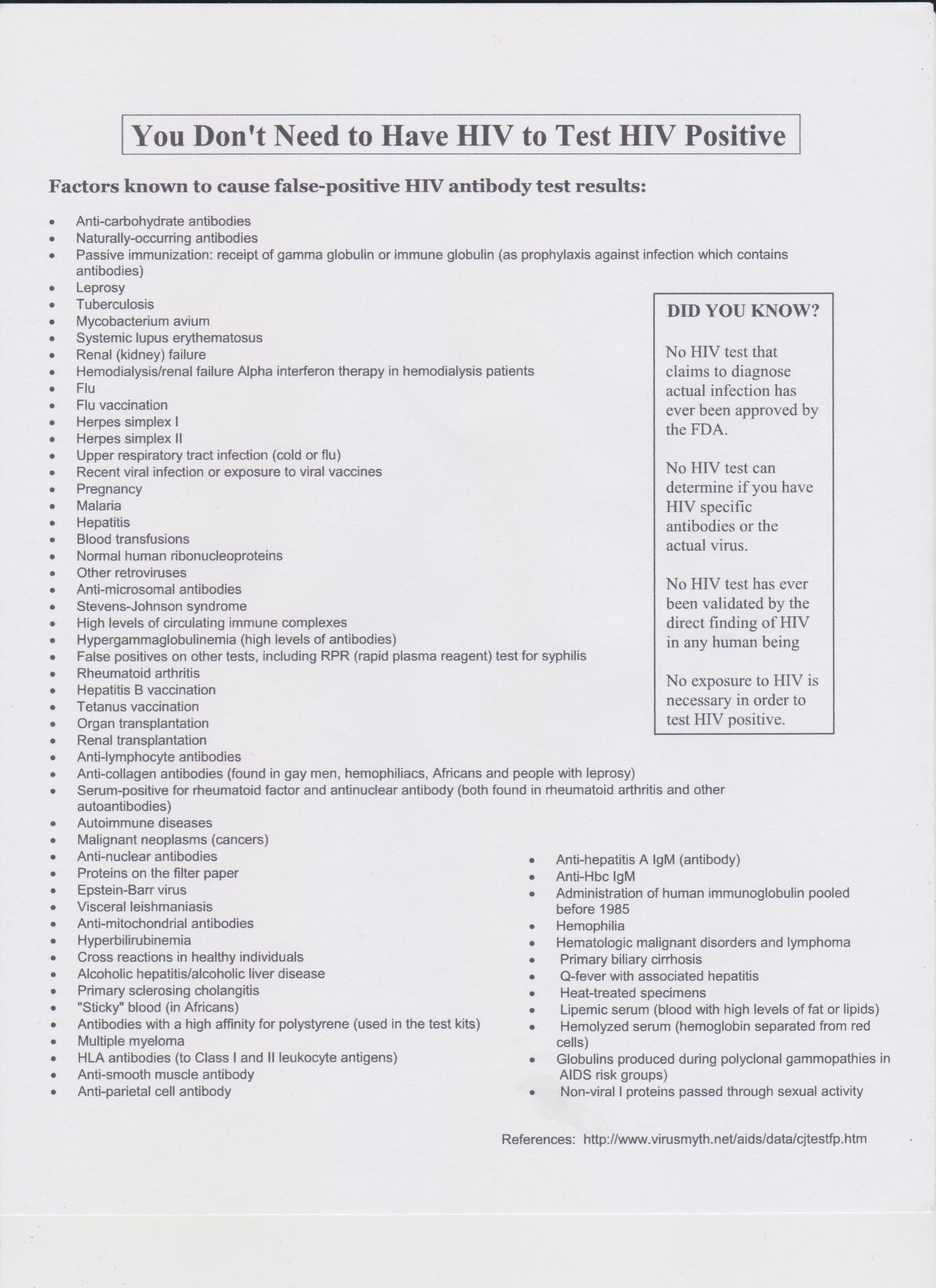
It is known that these antibody tests are non-specific, as there are over 60 conditions15 (such as pregnancy, tuberculosis, influenza etc.) that can trigger a positive test.
PCR:
Viral load measurements with the help of the polymerase chain reaction (PCR) are just as dubious and ultimately meaningless. Since HIV has never been purified and characterized as a whole unique structure, these tests cannot be calibrated for HIV – and they cannot be used to measure “HIV viral load”.
At no stage in the history of AIDS have the PCR been verified against HIV isolation/purification, that is, against the putative virus for which the tests are employed.
The PCR only looks for very small genetic snippets, it cannot detect a complete virus.
The notion that the fine traces of genetic material belong to a (certain) virus remains entirely unproven. PCR itself cannot identify the origin or significance of the small gene fragment which it detects.
CD4 cell count:
CD4 cells, also known as helper T cells, are a type of white blood cell that are said to help fight infection by triggering your immune system to destroy pathogens.
The HIV theory of AIDS is as follows: Viral infection → CD4 cell destruction → The clinical syndrome (AIDS).
However, not a single study confirms the most important principle of the HIV = AIDS theory: that HIV destroys CD4 cells by means of an infection. Researchers might point to an association between surrogate markers (said to be HIV) and the decline of CD4 cell counts.
However, as discussed earlier, these surrogate markers have never been proven to belong to HIV. Furthermore, association does not prove causation.
A low CD4 count is a common non-specific16 reaction to many kinds of physical and psychological stressors. A low CD4 count can be caused by a multitude of factors, such as; ‘viral’ infections, bacterial infections, parasitic infections, sepsis, tuberculosis, coccidioidomycosis, multiple organ system failure, burns, trauma, intravenous injections of foreign proteins, malnutrition, over-exercising, pregnancy, autoimmune diseases, pneumonia, leprosy, normal daily variation, psychological stress, social isolation, etc.
Thus making the explanation of a fictitious ‘virus’ as a culprit entirely unnecessary.
Enter AZT
Once the medical authorities declared that the multifactorial condition called AIDS was caused by a virus, they needed to come up with a way to treat it. In the late 1980’s, the pharmaceutical companies dusted off an old and very toxic drug, originally developed for chemotherapy, called azidothymidine (AZT), and remarketed it for use with AIDS patients.
Most cancer chemotherapies are administered as a short series of treatments, with rest periods in between each course to allow the patient’s system to recover from the effects of the toxic treatment. Conversely for AIDS patients, AZT treatments were to be taken for ‘life’, which, at the high doses that were initially prescribed, became extremely short.
Although these people are reported to have died from ‘AIDS’, the main contributory cause of their deaths was the highly toxic AZT treatment.
The medical community ignored the possibility of AZT-poisoning as cause of death, because their belief in the deadliness of HIV was so firm that they weren’t even shocked when patients died within a short time.
John Lauritsen described the AZT narrative in his book published in 1990, entitled Poison by Prescription: The AZT Story:17
“I imagine that future medical historians, looking back on the present, will regard many or even most of the AIDS fatalities as iatrogenic – caused by medical treatments rather than by AIDS itself (whatever exactly ’AIDS’ is).”
[...]
“The old rationale for prescribing AZT was that people with AIDS were suffering from a disease that was invariably fatal, that such people had only a few months to live, and that AZT might extend their lives for a few more months. The idea was that in a desperate situation, drastic measures were called for … Now a completely different game plan is in operation … physicians are now being urged to prescribe AZT for perfectly healthy people … Healthy people, who ought to look forward to living for several more decades, are now being conned into taking the most toxic substance ever prescribed for long-term use.”
References:
1HIV.gov. “A Timeline of HIV and AIDS”. https://www.hiv.gov/hiv-basics/overview/history/hiv-and-aids-timeline/
2Re-Solv. “Alkyl nitrites (‘poppers’)”. https://www.re-solv.org/volatile-substance-abuse/alkyl-nitrites-poppers/
3Mayo Clinic. “Kaposi's sarcoma”. https://www.mayoclinic.org/diseases-conditions/kaposis-sarcoma/cdc-20387726
4Alcohol and Drug Foundation. “What is amyl nitrite?”. https://adf.org.au/drug-facts/amyl-nitrite/
5HIV.gov. “What Are HIV and AIDS?”. https://www.hiv.gov/hiv-basics/overview/about-hiv-and-aids/what-are-hiv-and-aids/
6World Health Organization: Weekly Epidemiological Record no. 10-7 March 1986. https://apps.who.int/iris/bitstream/handle/10665/225716/WER6110_69-74.PDF
7Barré-Sinoussi, F et al. “Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS)”. Science. vol. 220,4599 (1983): 868-71. https://pubmed.ncbi.nlm.nih.gov/6189183/
8The Emperors New Virus? - An Analysis of the Evidence for the Existence of HIV. Time: 16:45. Page: 12. http://www.theperthgroup.com/OTHER/ENVCommentary.pdf
9Christine Johnson. “Factors Known to Cause False-Positive HIV Antibody Test Results”. Continuum Magazine Vol 4, No. 3. September/October 1996. http://www.tig.org.za/pdf-files/affidavit-aug06/54%20Factors%20known%20to%20cause%20false%20positives.pdf
Magazine PDF: https://www.immunity.org.uk/wp-content/uploads/2013/06/v4n3.pdf
10First image: Varmus H. (1988). “Retroviruses”. Science, 240(4858), 1427–1435. https://pubmed.ncbi.nlm.nih.gov/3287617/
Second image: Varmus H. (1987). “Reverse transcription”. Scientific American, 257(3), 56–64. https://pubmed.ncbi.nlm.nih.gov/2443971/
11O'Hara, C J et al. “The ultrastructural and immunohistochemical demonstration of viral particles in lymph nodes from human immunodeficiency virus-related and non-human immunodeficiency virus-related lymphadenopathy syndromes”. Human pathology vol. 19,5 (1988): 545-9. https://pubmed.ncbi.nlm.nih.gov/3371979/
12The four papers are:
First: doi:10.1126/science.6200935
Second: doi:10.1126/science.6200936
Third: doi:10.1126/science.6200937
Fourth: doi:10.1126/science.6324345
https://en.wikipedia.org/wiki/Robert_Gallo#cite_note-17
13Methods and data are reported in three papers:
First: doi:10.1126/science.6089333
Second: doi:10.1038/312166a0
Third: 10.1126/science.6095449
14Papadopulos-Eleopulos, E et al. “HIV – A virus like no other”. Posted at the Perth Group website July 12th 2017. www.theperthgroup.com/HIV/TPGVirusLikeNoOther.pdf
15Christine Johnson. “Factors Known to Cause False-Positive HIV Antibody Test Results”. Continuum Magazine Vol 4, No. 3. September/October 1996. http://www.tig.org.za/pdf-files/affidavit-aug06/54%20Factors%20known%20to%20cause%20false%20positives.pdf Magazine PDF: https://www.immunity.org.uk/wp-content/uploads/2013/06/v4n3.pdf
16Matt Irwin. (2011). “Low CD 4 + T lymphocyte counts : A variety of causes and their implications to a multifactorial model of AIDS”. http://virusmyth.com/aids/hiv/milowcd4.htm
17John Lauritsen. “Poison by Prescription: The AZT Story”. https://covidhoax.org/hiv/Poison-by-Prescription-The-AZT-Story.pdf
Great article. All the flawed science involved in the HIV/AIDs fiasco is so glaringly obvious when you set it out like you have.
Thank you for writing up about HIV & AIDS ... I have added the links to your articles here -
Is HIV a "virus" that causes AIDS?
https://hewettinsite.substack.com/p/is-hiv-a-virus-that-causes-aids